![]()
[Andrianne, BioMed, Dewit-Leunis, Heel, Henry, Piterà, Piterà2]
Diseases are not static disorders that do not change over time, but rather they have their own evolution. We can always describe the cause of onset of a disease in terms of an interaction of the body (with its specific constitution, its resilience and its predispositions to disease) with one or more “pathogenic” events (noxae), external or internal to the body itself (think for example of a “cold”, a virus or even a prolonged stress).
Several models, each with its own peculiarities, have been formulated which, starting from this general assumption, describe the evolution of diseases. Of particular interest are the models offered by gemmotherapy and homotoxicology because they allow us to evaluate the stage of the progression of any kind of morbidity in both acute and chronic cases, thus providing the tools for a classification and treatment of diseases according to the stage. It is interesting to note that, despite the considerable differences from both a theoretical and a diagnostic and therapeutic point of view, the two models share several common points, so much so that they can made almost overlap once the appropriate considerations and clarifications have been made.
The phases
Homotoxicology ([Andrianne, Heel, Reckeweg]) and gemmotherapy ([Andrianne, Dewit-Leunis]) propose a six-phase evolution scheme for chronic diseases. Both schemes start from the body’s encounter with a generic noxa. In homotoxicology, noxae take the specific name of homotoxins.
Activation or excretion phase
Any disease starts when a living organism comes into contact with an “entity”, be it chemical, physical or biological, external to the organism or internally produced, that is at least potentially pathogenic. In the event that this entity is not dangerous for the organism, the latter simply does nothing; if, on the other hand, the entity constitutes a danger (in this case, we speak properly of noxa, pathogen, toxin), after this contact the organism always puts in place a form of reaction.
In the first reaction phase, called activation or phase I by Dewit and Leunis and excretion by Reckeweg, the body tries to remove the pathogen simply by increasing its secretions and physiological excretions. It is an almost passive management strategy that does not produce the typical clinical manifestations of defense reactions. In this phase, the toxins do not interfere, for example, with the epithelial cells of the mucous membranes but are incorporated in and eliminated through the physiological fluid secretions (sweating, diarrhea, vomiting, tears, urine, ear wax, catarrh, etc.), which may be temporarily increased. This phase covers all hyper-secretions (endocrine) and hyper-excretions of the various organs and tissues. The expulsion of toxins occurs through the orifices of the body (this reminds of the concept of “opening of the pores” of some traditional medicines). If the removal of the pathogen is successful, the body spontaneously returns to equilibrium without any insult.
Since this is a phase in which the reaction consists exclusively in an overproduction of liquids or in the fluidification of the secretions and excretions, from the humoral point of view it can be considered a mainly phlegmatic phase, in which the Phlegm is typically mobile and not thickened.
|
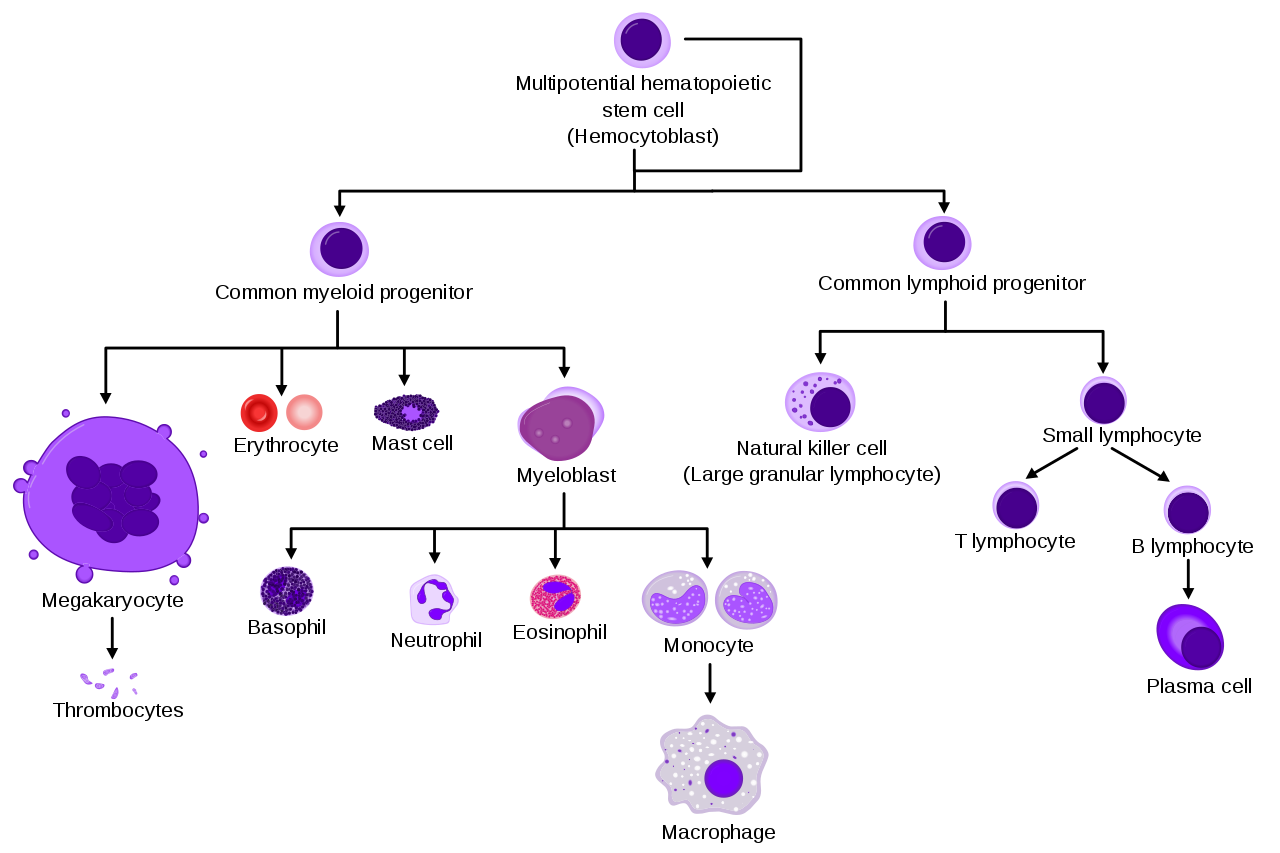
Notes on the immune system [Cheng, Dixon, Roggel, Wikipedia] Blood cells are all produced from hematopoietic stem cells[i] (HSC) that reside in the bone marrow, through a process called hematopoiesis. The details of this process have not yet been fully clarified, and several alternative models still co-exist. For our purposes, it is sufficient to take into consideration the so-called classical model, which, despite having several criticalities, still guarantees a good understanding of the “phylogenetic” relationships between the different cell lines. HSC cells are able to self-renew and are pluripotent, that is, they are capable of generating genetically different daughter cells (lineages). The process that leads to the formation of mature blood cells is a hierarchical process which, starting from the hematopoietic cells, produces cells that progressively lose the ability to self-regenerate, proliferate and give life to different cellular lineages (lineage potentials). Broadly speaking, according to the classical model, the mitotic division of HSC leads to the simultaneous formation of two types of cells (asymmetrical division), namely:
A series of steps controlled by the presence of different growth factors (including erythropoietin, thrombopoietin, some interleukins and the various colony-stimulating factors) leads to a further differentiation of the pluripotent cells into two types of progenitor cells, that is:
All blood cells derive from these two types of progenitor cells. For this reason, blood cells can be divided into two large classes (see fig. 1):
Granulocytes (or polymorphonuclear leukocytes[ii]) and monocytes both originate from the myeloblast (see fig. 1). Monocytes can in turn differentiate into macrophages and myeloid dendritic cells. Langherhans cells are tissue macrophages located in the skin (in all layers but especially in the stratum spinosum), while Kupffer cells (or stellate macrophages) and Kupffer-Browicz cells are liver resident macrophages. Kupffer cells accounts for 80–90% of all tissue macrophages present in the body.
Fig. 1 – Blood cell lineages [Häggström] Histiocyte (from the Greek ἱστός, istòs, which means tissue and which is used to indicate an organic tissue, and –cyte, a suffix that derives from the ancient Greek κύτος, kytos, which indicates a cavity filled with liquid, and is used to denote cells) is the name given to any cell that is part of the mononuclear phagocytic system (MPS, also known as the reticuloendothelial system or lymphoreticular system). Histiocytes can be either tissue macrophages or dendritic cells. However, the term histiocyte has been used in the past for several purposes and some cells called “histiocytes” do not derive from monocytic-macrophagic lineages. Globulins are a family of globular proteins with a molecular weight higher than albumin. They are insoluble in pure water but soluble in dilute salt solutions. Some globulins are produced by the liver, while others are produced by the immune system. Globulins, albumins and fibrinogen are the main blood proteins. The normal concentration of globulins in human blood is approximately 2.6-3.5 g/dl. The term “globulin” is sometimes used as a synonym for “globular protein”. In fact, albumins are globular proteins too, but they are not globulins. All other globular serum proteins are globulins. All globulins fall into one of the following four categories: α1, α2, β and γ. One group of γ-globulins is that of immunoglobulins, also known as “antibodies”. Globulins can be separated from each other by means of electrophoresis of serum proteins. |
Inflammation phase
If the first attempt to remove the pathogen fails (because the excretory abilities of the body are insufficient or because the aggressor is too strong and challenges the host’s possibilities of adaptation) and the pathogen manages to reach the extra-cellular and/or intracellular levels, the body begins to mount some form of local defense reaction to counteract the “toxic state”. The first defense lines (innate immunity) are activated and an inflammatory condition arises that involves first the granulocyte cells (mainly neutrophils).
Depending on the degree of infiltration of the polymorphonuclear cells, an exudative phenomenon may occur that may re-enter (the tissues appear infiltrated by neutrophils and eosinophils, with a serous exudate that is especially rich in type-α glycoproteins, which can induce hypersensitivity reactions, such as allergies, and even be able to cause serous extravasation or production of acute mucous catarrhs, as in cases of coryza, gastroenteritis, tracheitis, bronchitis, colitis, etc.), or a suppurative phenomenon may take place that must find a way out of the body. Suppuration produces organic material consisting largely of neutrophils or eosinophils.
This phase is called exudative inflammation phase by Dewit and Leunis and is characterized, from the cellular point of view, by the activation of the myelocyte defense line and by microcytic phagocytosis[iii] and, on electrophoresis, by an increase in the α-globulins, a group of anti-inflammatory proteins such as haptoglobin (Cetavlon test +), α2-macroglobulin, antichymotrypsin, ceruloplasmin[iv]. For this reason, it is also called hyper-α phase in gemmotherapy. Five parameters are used in gemmotherpay to study this phase: the globulin patterns detected by electrophoresis, the LPI[v] profile of the euglobulins of the reticulo-endothelial system, the Cetavlon test, the copper acetate test, the cadmium test.
All acute forms of inflammation fall into this phase. Insect bites, sunstrokes, laryngeal-epiglottal edema, lung edema, acute brain edema, acute interstitial nephritis, burns are all phenomena related to this exudative phase, which tends to evolve towards sclerosis by secondary lymphoplasmacytic reaction. If there is plasma exudation, the inflammation is no longer considered exudative but fibrinous due to the precipitation of fibrin: this is the case of fibrinous pleurisy, fibrinous pericarditis, fibrinous peritonitis or fibrinous pneumonia[vi].
Globulins not only represent the body’s tendency to defend and immunize against infections, but also the response to chronic inflammation and chronic tissue infiltration. The increase in the α1 and α2 fractions corresponds to an attack on the liver cell by a bacterial or viral infection, a violent trauma or a thermal shock. It is an organic response to an acute, non-specific event that mobilizes the leukocyte line of white blood cells. These modifications are therefore due to acute inflammation. The more α1 and α2 increase, the more severe the inflammation is and the more the albumins are likely to decrease, further aggravating the prognosis. For example: in case of pneumonia a net increase in α1 and α2 occurs, but a decrease of albumins during the course of the disease can indicate that we are facing a spread of the inflammation, that may have extended to the pleura with a possible pleuropneumonia.
At a later stage, cells of the histio-monocyte lineage (monocytes, macrophages and dendritic cells) can be mobilized. From the tissutal point of view, this corresponds to the onset of congestion: this corresponds to a local vascular reaction that stimulates the histiocyte defense or that can cause macrophage phagocytosis which is intended to limit the reaction or to inform the body’s immune sytem. This phase, which, citing Pol Henry, can be called the congestion phase, from the point of view of electrophoresis is mainly linked to β-globulins. For this reason, it is defined by Dewit and Leunis and by Andrianne as hyper-β or steatotic phase[vii].
Here the authors differ slightly:
- Dewit and Leunis place the hyper-α phase between the end of the activation phase and the beginning of the reaction phase (end of phase I and beginning of phase II) and the hyper-β phase completely in the inflammation phase (phase II);
- Andrianne places the hyper-α phase in the exudative phase (activation) and at the beginning of the reaction phase (phase I and early phase II) and the hyper-β phase together with the hyper-αβ phase (but subsequent to the latter) in the exudo-steatotic phase, between the inflammation phase and the subsequent deposition phase (phase II and early phase III);
- Pol Henry does not even mention a specific hyper-β phase[viii].
Since the work by Dewit and Leunis is more recent, we refer to the classification of the latter two authors, with the only difference that we put the hyper-α phase completely in the reaction phase, since the activation phase does not involve the immune system[ix].
Thanks to the action of monocytes and histiocytes, the “deposition” of the information related to the typing of the aggressor also begins. The immune system, indeed, will keep memory of this conflict (the macrophages and, even more, the dendritic cells phagocytize the aggressor and present some “pieces”, the antigens, to the T lymphocytes which have the task of memorizing the antigens, recognizing them and responding to their presence).
Both the phases just described constitute, together, the phase called inflammation phase in homotoxicology and inflammation or reaction phase by Dewit and Leunis.
The activation of phagocytes and phagocytosis should be seen as the first reactive step of “detoxification”, and inflammation can be considered a process aimed at “cleaning” the extracellular matrix (the cell is not yet directly involved, although inflammatory processes may passively damage it). Therefore, the symptoms, however annoying, are important signs of the body’s attempt to heal. It is rarely necessary or helpful to suppress fever and acute inflammation with allopathic drugs, such as anti-inflammatories and antipyretics. The use of antipyretics and drugs that suppress cough, diarrhea, etc., can lead to what in homotoxicology is called progressive vicariation, that is, to an advancement of the disease.
From the point of view of humoral medicine, inflammation is a phenomenon linked to the Bile humor. It is interesting to note that, especially in the exudative phase, the α-type globulins play an essential role: these are mostly anti-inflammatory proteins produced by the liver, the depositary of the biliary “function” and of the production of Bile (also in the humoral sense). In the second part, β globulins are more involved: these proteins are co-responsible for the subsequent organ steatosis, that occurs when the tissues are overladen of macromolecular particles (lipid and protidic macromolecules), and these, no longer able to remain in the colloidal equilibrium of the serum, precipitate into the tissues. If the inflammatory “origin” of this phase is, as mentioned, linked to the Bile humor, its tissutal manifestations often have a phlegmatic component: if this is immediately evident with the exudative inflammation, even during the suppurative inflammation (corresponding to the “toxic heat” of Chinese medicine and understood as a perverse form of heat-dampness in Hippocratic-Galenic medicine) the production of a phlegmatic excretion occurs, although this is “thickened” from the presence of phlegmatic-melancholic particles (the granulocytes, which are both “white” and corpusculate). The hyper-β congestion phase can be directly described as a local, “tissutal” stagnation of the Blood humor (not to be confused with the Blood stagnation of Traditional Chinese Medicine, which is much more advanced in the sense of the progression of the phases).
Deposition and impregnation phases: exudo-steatosis, fibrinosis, hyalinosis
If it is unable to eliminate the aggressor directly and completely by excretion through fluids and/or by suppuration, the body moves on to a new phase: the noxae and the macromolecules involved in the immune process (cholesterol, proteins, …) now exceed the coping ability of the body, and so they are temporarily stored in the tissues, so that they can be managed at a later, more favorable time[x]. This can happen for several reasons, such as:
- the inflammation process (previous phase) was not adequately activated or was blocked/suppressed (for example, by drugs administered to suppress inflammatory symptoms);
- the excretion ability of the body is hypofunctional or the toxic load is excessive.
The point of view of homotoxicology: deposition and impregnation
According to homotoxicology, at this point the so-called deposition phase begins, in which regulation disorders and events that are internal to the extracellular matrix (ECM) predominate. It is a relatively silent process with very few clinical signs and symptoms, but nonetheless it is quite a dangerous process. In fact, it is only a matter of time before the homotoxins manage to reach the inside of the cell or interfere with the cell from the outside, altering or even preventing its normal functions.
During the deposition phase, the toxins that the body is not able to excrete are deposited into the connective tissue, the adipose tissue and the vascular system. Cellular metabolic functions need to be stimulated so that they can be restored and supported in the release and gradual expulsion of toxin deposits.
When the concentration of the homotoxins deposited in the tissues becomes so important as to “impregnate” the extracellular matrix or to produce intracellular effects, the impregnation phase begins. At this point, the homotoxins have practically become part of the structural components of the connective tissue and the matrix. Some toxins (for example, viruses, which, unlike bacteria, are to be considered “real” homotoxins) can penetrate directly into the cells of the connective tissue or parenchyma. The toxins that reach this stage begin to induce functional changes both in the matrix and in the cells, for example by interfering with enzymatic processes and metabolic pathways, by damaging cell membranes, by compromising the mitochondrial respiratory chain, etc.
These alterations lead to less efficient cellular functioning, and the body’s reactions to homotoxins are often no longer resolutive. Sometimes, a minimum load of a specific homotoxin induces the body’s defense mechanisms to a hyper-reaction (asthma, hay fever, migraine, gastric ulcer, …). From the histological point of view, some structural changes begin to appear, while, from the clinical point of view, signs and symptoms indicative of cell damage begin to appear. The impregnation phase can be reached in a rather short time, mostly depending on the characteristics of the homotoxins. Many viruses attempt to penetrate the host cells and to replicate rapidly, and although the body tries to develop a specific defense (immunoglobulins) and to eliminate infected cells (T-cell activity and NK-mediated cell elimination), the acute condition is in fact an impregnation phase due to the intra-cellular presence of viruses. Even if the tissues are completely repaired and the damaged cells are all replaced, the viral condition still remains in the impregnation phase if the virus has been “incorporated” into the genetic material of the host cell. In post viral syndromes this situation can persist for a long time, even for years.
In the impregnation phase, a “locus minoris restistentiae”[xi] is created: the accumulation of toxins around the organ parenchyma generates an inflammatory response aimed at attempting to isolate the toxins (and the inflammation itself) within the biologically less important tissue, namely the connective tissue. If the accumulation of toxins continues and they are not removed in some way, the inflammation progresses, leading to the degeneration of the organ structure.
Between the deposition and the impregnation phases, the so-called Regulation/Compensation Division (or “biological division line”) is placed, which separates the first three phases (excretion, inflammation, deposition) in which the elimination of toxins is still possible in simple ways (and therefore the body is still able to heal autonomously or, at most, only needs to be supported by appropriate therapy) from the last three phases (impregnation, degeneration and dedifferentiation) in which excretion is no longer obtainable (at least spontaneously). In the first three phases, the cellular biochemical mechanisms have not yet been damaged, but, passing from the deposition phase to the subsequent impregnation phase, the body begins to no longer have efficient biological defenses and starts to “withdraw” energy from the process of detoxification, in order to preserve it for the functioning of vital organs: at this point, the penetration of cells by toxins begins.
The point of view of gemmotherapy: deposition, fibrinosis and hyalinosis
According to gemmotherapy, in the phase following the failure of the inflammatory reaction, the immune system expresses by rising specific markers, which can be found among the proteins of the α and β-globulins group, but also works to “keep memory” of the unresolved conflict in order to be able to handle a similar condition in the future. It is in this phase that allergic sensitizations occur and that the signs of cellular hypoxia and steatosis of the noble organs appear. This is the so-called deposition or exudo-steatotic phase, (see [Andrianne] and [Dewit-Leunis]) that is characterized by a hyper-αβ-globulinemia and which corresponds (at least from a “qualitative” point of view[xii]) to the deposition phase of homotoxicology.
In the next two phases, called fibrinosis (hyper-αγ) and hyalinosis (or scleroyalinosis, hyper-αβγ), the transition to a more specific involvement of antibody proteins (γ-globulins) occurs.
The fibrinoid degeneration, which is linked to the degeneration of the fibers of the connective tissue (and to a possible involvement of fibrin), is found in allergic inflammation and in a whole series of collagenous tissue alterations. The hyaline transformation, which is characterized, from a morphological point of view, by the presence of an amorphous substance with a homogeneous vitreous appearance in the sections colored by eosinophilic staining, is a form of sclerosing infiltration of the organs that causes hypertrophy of the supporting tissues and atrophy of the parenchyma, and therefore begins to be insidious (it is, among other things, the basis of cellular or physiological aging). If the exudative, steatotic and fibrinosic phases are considered primary, the hyalinization of a tissue represents a more advanced phase, secondary to a previous fibrinosis.
According to Pol Henry, the increase in γ-globulins signals that tissues are definitively affected by an attack that will leave an indelible mark. With the onset of the hyper-γ phases, chronic inflammation begins[xiii] and it is no longer possible for a natural, spontaneous resolution of the progressive pathology to occur[xiv].
Dewit and Leunis speak of a phase III or deposition phase and a subsequent phase IV or fibrosis phase. These two phases can be made to correspond to the impregnation and degeneration phases of homotoxicology, respectively. It is interesting to note that Dewit and Leunis place fibrinosis (hyper-αγ) within the phase III (deposition) and only at the beginning of phase IV (fibrosis), while Andrianne places it completely within phase III. The hyalinosis phase (hyper-αβγ) is the one that most completely belongs to the fibrosis phase (IV): here, a real protein degeneration occurs that modifies the parenchyma and the supporting tissues. At this point, according to the authors, tissue degeneration is definitely irreversible.
Since:
- the homotoxicological and the gemmotherapeutical models differ here for nuances (the fibrinosis phase is placed completely in the deposition phase, part in the deposition and part in the fibrous phase, or even completely in the fibrosis/impregnation phase);
- there is obviously a continuum of evolution from fibrinosis to hyalinosis, reason why, in reality, the phases are not clearly defined;
- fibrinosis already produces an important alteration of the connective tissue, with ever increasing damage to the parenchyma as hyalinosis approaches;
- fibrinosis is characterized by the involvement of γ-globulins, reason why it is already a “chronic” and irreversible condition (according to what Pol Henry asserts)
in this text, fibrinosis is formally placed entirely in phase IV, making the phase of fibrosis of Dewit and Leunis coincide with the impregnation phase of homotoxicology, aware of the fact that we are however referring to a continuum with respect to the evolution of the extracellular matrix, which is increasingly damaged by the already chronic inflammatory process.
Tissutal acidification and deposition
Any phenomena that interfere with the circulation of fluids within the extracellular matrix (including a lack of water, nutrients or physical activity), if not resolved, can lead to a reduction in lymph movement and congestion of the ECM, resulting in reduction of the elasticity of the matrix. This can induce a slowdown both in the transport of oxygen, nutrients and biochemical messengers, and in the elimination of waste products. In the long run, these conditions can produce hypoxia, which, together with the accumulation of waste products, can induce tissutal acidification (decrease in interstitial pH), which in turn can result in a stiffening of the matrix and connective tissue, which further worsen the movement of fluids, thus establishing a vicious circle (see box below).
|
Hypoxia, acidification and fibrosis[xv] Hypoxia, acidification and fibrosis are phenomena that, at the tissue level, normally occur during tissue repair (for example, during wound healing) and are physiological in the acute cases; however, these processes can also be involved in the establishment and progression of chronic diseases. Tissutal hypoxia and tissutal acidification can be linked to each other through the increase in cellular glycolytic metabolism in hypoxic areas. When hypoxia occurs in mammalian tissues (eg, due to tissue damage), a whole cascade of events is induced to react to the decreased oxygen availability. Under such conditions, transcription factors known as HIF (Hypoxia-Inducible Factors) are activated. HIF-1α is considered the main transcriptional regulator of the cellular response to hypoxia. According to what is known so far, it induces the transcription of more than 60 factors, including VEGF and erythropoietin which are involved in biological processes such as angiogenesis and erythropoiesis, which have the task of facilitating the transport of oxygen toward the hypoxic regions. HIF-1α also induces the transcription of genes involved in cell proliferation and survival, as well as in glucose and iron metabolism. Some types of activated immune cells, including macrophages, prefer to use glycolysis for energy production (Warburg effect) even in normoxic environments. It seems that anaerobic glycolysis is specifically promoted by the pro-inflammatory activation of immune cells and not by their anti-inflammatory activation; classically activated pro-inflammatory M1 macrophages and T cells show a glycolytic phenotype, whereas alternatively activated M2 macrophages and regulatory T lymphocytes with anti-inflammatory properties are characterized by increased oxidative phosphorylation [Öörni]. HIF-1α is essential for the regulation of glycolytic capacity in all myeloid cells [Crame, Walmsley]. Macrophages located in hypoxic areas can be stimulated to effect a HIF-1α-dependent increase in glycolytic metabolism. As with macrophages, pro-inflammatory activation of dendritic cells via toll-like receptors and activation of T lymphocytes via T cell receptors also cause a HIF-1α-dependent increase in glycolytic metabolism [ Öörni]. Granulocytes contain abundant mitochondria and have the ability to maintain aerobic metabolism, but however they rely almost exclusively on anaerobic glycolysis for ATP generation, as they need to move within environments that are poor in oxygen. HIF-1α again provides the key mechanism for regulating granulocyte glycolysis, but, in this case, it also stimulates (together with the macrophage inflammatory protein-1β) a reversible inhibition of neutrophil apoptosis which prolongs their survival, thus increasing their activity [Walmsley]. The excess of H+ and lactate produced by the increased glycolysis is secreted by the cells into the ECM through various pumps, exchangers and transporters, locally decreasing the pH of the cellular environment (interstitial pH). Macrophages are able to adapt and survive to the local acidosis that develops in the sites of acute inflammation and are subject to acidosis-induced modulation of their immune functions. Noteworthy is the fact that extracellular acidity also decreases the intracellular pH of macrophages, and this greatly amplifies the number of pathways potentially modulated by extracellular acidosis. The low pH modulates the activity of macrophages and monocytes, stimulating their uptake of immune complexes, the clearance of apoptotic cells and the presentation of antigens, and increasing the production of ROS species; it also stimulates the secretion of key pro-inflammatory cytokines (such as IL-1β and IL-18). Thus, an acidic environment has a strong pro-inflammatory potential [Öörni]. Although these effects may be beneficial in ensuring efficient clearance of acute inflammations, they become maladaptive in the context of chronic conditions. Indeed, an ECM acidity that persists over time is linked to the establishment and progression of chronic diseases, such as asthma, atherosclerosis and even cancer. A chronically decreased ECM pH can also promote structural changes in the surrounding tissues. Connective tissue growth factor (CTGF) is a cysteine-rich 38-kD protein that is now considered a key mediator of tissue fibrosis. It has been verified that low pH alone has the ability to induce a substantial production of CTGF and to increase the expression of both CTGF mRNA and protein induced by TGF-β (see for example [Matsuzaki]). High levels of TGF-β and CTGF are associated with a pathological deposition of ECM proteins that lead to an increase in tissue stiffness. Results from both in vitro and in vivo experiments showed an increased production of ECM proteins, including fibronectin, collagen, elastin and matrix proteoglycans, following stimulation with TGF-β and LPA (lysophosphatidic acid). This mechanism can cause matrix stiffness, which, in turn, induces the differentiation of myofibroblasts through a mechanism mediated by intrinsic mechanotransduction. The stiffening of the matrix and the thickening of the connective tissue can obviously cause a deterioration in the circulation of fluids which further increases hypoxia. |
During the deposition phase, the progressive accumulation of noxae and of lipid and protein particles within the connective tissue increasingly hinders the movement of tissue fluids. In the long run, this can induce hypoxia and therefore lead to the establishment of the vicious circle of hypoxia-acidification-stiffness. It is possible that the transition from the deposition phase to that of impregnation goes (also) through the activation of this vicious circle and of the related inflammatory mechanisms.
Comparison between models and the humoral point of view
The phases that follow the exudative inflammatory phase are characterized, according to both gemmotherapy and homotoxicologicy, by an increase in the complexity of the body reaction.
There is a good correspondence between the homotoxicological deposition and impregnation phases and the deposition, fibrinosis and hyalinosis phases of gemmotherapy. It is important to consider that:
- The deposition phase is common to both models: in this phase, the homotoxins are stored in the connective tissue together with the serum macromolecules, no longer soluble. This is a phase of “pure” storage, without particularly evident reactions and clinical signs.
- When the accumulation of toxins starts to be particularly important, the impregnated tissues begin to react to the toxins deposited in them: the toxins begin to interfere with the cells of the parenchyma, damaging their enzymatic functions and possibly also the membranes. This is where the impregnation phase begins. In this phase there is a “locus minoris resistentiae” [BioMed], whereby the chronic inflammatory process starts in a “biologically less important tissue” (connective tissue), but the side effects are equally important: the toxins collect around the organ parenchyma, the tissues react to these toxins with inflammation trying to isolate them within the connective tissue fibers, and, in the end, this process damages the organ as a whole.
- According to gemmotherapy, the phase following deposition is characterized by an increase in γ-globulins, indicators of the chronicization of inflammation. Thus, fibrinosis, which is the first hyper-γ-globulin state, is already a state of chronic inflammation. For this reason, we can affirm that the state of fibrinosis corresponds to the first part of the impregnation phase, while hyalinosis, although belonging to the same phase, represents a more advanced condition. On the other hand, however, according to gemmotherapy, hyalinosis is a hyperplastic rather than hypoplastic process (and therefore it is not yet degenerative), just like fibrinosis[xvi].
- The substantial difference between the deposition, impregnation and degeneration phases is that in the first phase storage of materials occurs without an inflammatory reaction, in the second phase a (chronic, at this point) inflammatory response is triggered due to excessive accumulation of such materials, but without a direct (important) involvement of the parenchyma, and in the third phase also the parenchyma is damaged, in a functional and/or structural sense. So, for example, the deposition of amyloid protein in brain tissue, the consequent chronic inflammation and the resulting degeneration respectively correspond to the three different tissue phases, of which only the third corresponds to overt Alzheimer’s. Cirrhosis, too, can be thought of as occurring in several stages: deposition (e.g. hepatic steatosis), formation of fibrous tissue with inflammation but without degeneration of the parenchyma (which could correspond at least to the early stages of compensated cirrhosis) and finally degeneration of the parenchyma.
Thus, with the impregnation phase, the chronicization of the disease begins. The deposition of any type of substance, the resulting tissue hyperplasia (e.g., increase in adipose or fibrous tissue) and the subsequent chronic non-resolving inflammatory response constitute the response to a change in the coping strategy carried out by the body against the pathogen; this change is essentially aimed:
- at confining (at least temporarily) the aggressor, no longer directly attackable, into a limited area, and
- at redirecting the “energies” towards the restoration of the main body and tissue functions and the “simple” containment of the unthwarted threat.
From the humoral point of view, these phases and the processes that characterize them can be described in terms of transformation of the Phlegm humor. This, which in the excretion phase is produced in greater quantities in order to remove the pathogen, is subsequently heated up by the heat of inflammation, finally producing toxic heat or “accumulating” (together with heat), as a component of the Blood humor, in congestion[xvii]. If the warming up continues, the tissue Phlegm is “cooked” until it becomes “adust” and thickened (deposition phase). As the “coction”[xviii] continues further, the Phlegm “condenses” more and more, hardening and structuring, finally acquiring typically melancholic characteristics[xix]. In this way, an increasingly “harder” hyper-production is obtained (fibrinosis and then hyalinosis, the second more “structured” than the first).
So, from a humoral point of view the deposition phase is characterized by accumulation of thickened phlegm in tissues. It is important to note that thickened Phlegm is not formed exclusively due to chronic inflammatory phenomena, but it can also be produced as a result of acute problems (think, for example, of the inflammatory diseases of the respiratory system). In the latter cases, however, the thickened Phlegm tends to collect into the body’s natural cavities and not to deposit into the connective tissue, as occurs instead during the deposition phase[xx].
According to the traditional humoral medicine[xxi], Phlegm accumulation generates compression that in turn produces heat. Indeed, if during the previous phase we only found thickened Phlegm, during the impregnation phase we also find a certain amount of perverse melancholy that was produced by the “cooking up” of Phlegm (thickened Phlegm and perverse Melancholy together give reason for the hyperplasia that is typical of this phase). In a certain sense, the heat produced may be related to the renewed activation of the reaction processes (this time linked to the γ-globulins) of the body.
Degeneration phases: cirrhosis, fibrosclerosis
If the pathogen is not defeated, the body defense system is no longer able to remove toxins from the cells and/or the matrix. When this happens, the intracellular structures (genetic components, cell membranes and internal systems of the cell) begin to be affected and are subsequently more and more seriously damaged. According to both homotoxicology and gemmotherapy, at this point the degeneration (or necrosis) phase begins, that is, a phase in which cell damage is predominant.
According to homotoxicology, the progressive intoxication of the cell and of the surrounding tissues causes a complete functional failure of the affected cells which tend to progressively die. In the long run, tissue loss and functional limitation of all affected tissue appear. By definition, the degeneration phases are related to chronic degenerative diseases, most of which are to be considered irreversible.
According to the gemmotherapy model, all phases up to and including hyalinosis correspond to cellular hyperplasia and can be considered reversible from the point of view of both the tissues and the serum proteins. After the hyalinosic phase, Dewit and Leunis insert a stop phase: the body has not been able to stop the aggressor, so a necrotic phase of cellular hypoplasia (corresponding to the death of cells) begins which is meant to “radically” cleaning the tissues, trying to eradicate the pathogen. The phases following hyalinosis are to be considered irreversible from the tissutal point of view: even if the serum proteins can normalize, the disease will leave an indelible mark on the body’s tissues.
Schematically, the necrosis phase is put after the impregnation phase because of the greater extent of the damage, but, in fact, necrosis does not necessarily follows impregnation chronologically. Rather, which of these two phases is entered essentially depends on the pathogenic power of the aggressor[xxii]. Indeed, a necrotic lesion can also result directly from the conflict between the individual and a noxa when the latter is too “destructive” or too “hypoxic”, so as not to leave the individual the material time or the resources for the reconstruction of a scar.
In gemmotherapy, the degeneration phase is further divided into two successive stages. During the first of these, α-globulins decrease so that a hyper-βγ-globulinemia remains, sign of a cirrhotic drift (cirrhosis)[xxiii],[xxiv] of the disease. On the other hand, the increase in β-globulins may not occur at all or may be depressed over time: then only an isolated hyper-γ-globulinemia remains, evidence of a hyperimmunity syndrome, while the disease evolves toward the fibrosclerosis of the inflamed tissues, which is a further, more advanced phase of the proteic reaction process.
From the humoral point of view, the combustion of humors due to chronic and progressive overheating leads to the exhaustion of the organic material: we go from a phase of hyperproduction of (albeit perverse) Melancholy, typical of the previous states, to a state of Melancholy deficiency (always accompanied by the presence of a more or less important share of perverse Melancholia). The stop phase marks the transition from an excess of Melancholia to a deficiency of Melancholia[xxv].
Dedifferentiation phase: amylosis
If the hyper-γ-globulinemic syndrome typical of fibrosclerosis is depressed to produce a hypo-γ syndrome, we are facing an immune deficiency which, if isolated, is not always the consequence of a post-inflammatory stage (it may also be a primary or genetic deficiency, or, if it is accompanied by an increase in α- and β-globulins, it may indicate the terminal phase of an old inflammation, which however entails the risk of renal permeability with consequent signs of nephrosis due to albumin leak). The post-inflammatory hypo-γ stage, in gemmotherapy, is called amylosis (or scleroamylosis) and is considered a stage of degeneration or disorganization.
This phase occurs when, once all attempts to eradicate or contain the pathological process have failed, the host organism has no other way out than self-destructing through total disorganization of its vital functions. This is a state of disorganization typical of all processes that have anarchic developments, from acquired immune diseases, to hypothalamic-pituitary dysfunction syndromes up to benign and malignant tumors.
In homotoxicology, an analogous phase, called dedifferentiation, exists, which includes all diseases characterized mainly by abnormal cell proliferation or tissue growth. The cells lose their specificity and dedifferentiate to become totipotent cells (inverted embryonic specificity). These diseases can also be characterized by the presence of metastases. In this phase, the body is also increasingly influenced by endogenous toxins that are generated by cell destruction. All malignant tumors belong to this stage.
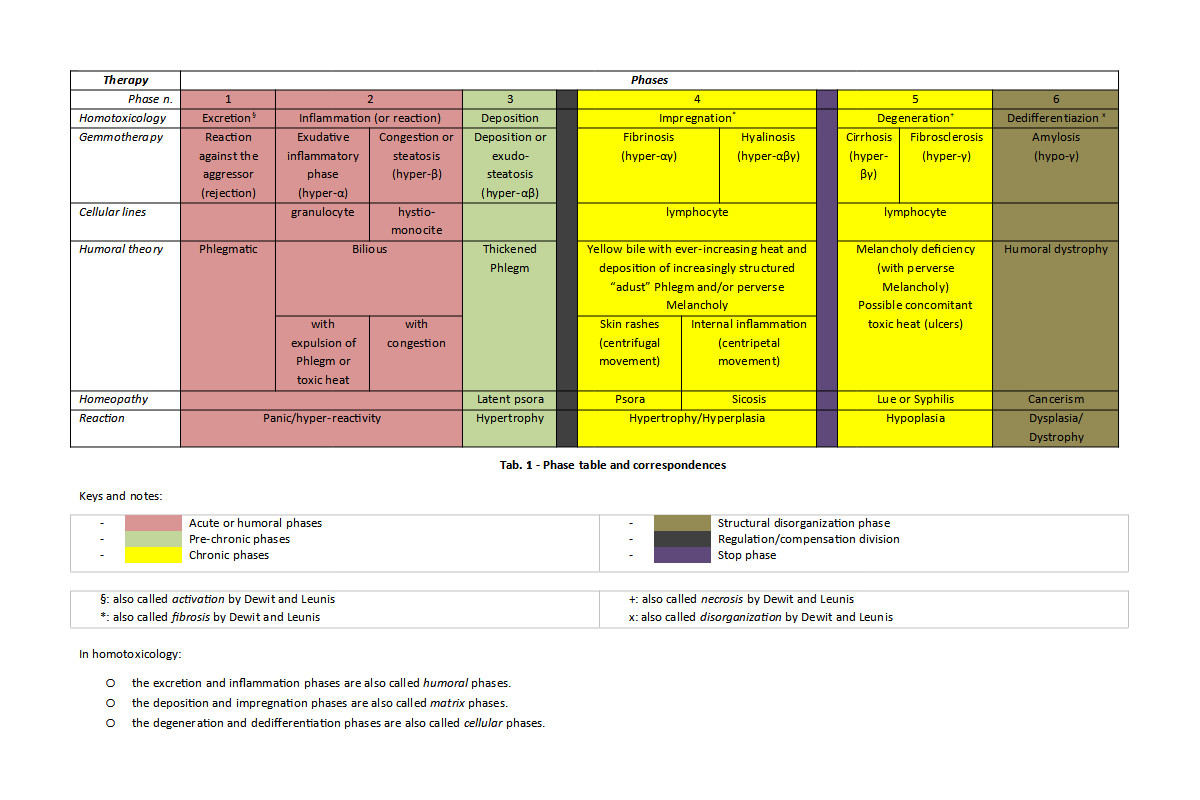
The phase table
Tab. 1 shows the summary of what has been said so far. Here, the phases of homotoxicology and gemmotherapy are made to coincide exactly for clarity sake, but it is important to understand that their correspondence is only qualitative. Gemmotherapy, in fact, defines the phases in terms of measurable biological parameters (serum proteins), whereas in homotoxicology no instrumental parameters are used at all. This means that, in practice, the accuracy of the correspondences cannot even be verified experimentally. Rather, since both models rest on the same sequence of events, it is reasonable to expect a rather accurate qualitative correspondence[xxvi]: it is possible, for example, that hyper-αβ activation is the cause of the initiation of deposition phenomena, or rather that hyper-αγ is consequent to the beginning of the impregnation phenomena. In this way we also abstract from the small differences between the opinions that the different authors (in gemmotherapy) have regarding the positioning of the reactions of serum proteins with respect to the tissue phases[xxvii].
It should be noted that if the impregnation phase is considered irreversible by homotoxicology, the corresponding phases of fibrinosis and hyalinosis are reversible according to gemmotherapy. In reality, this difference is only apparent, as they are all to be considered spontaneously irreversible, i.e. they require appropriate external intervention (therapy) so that tissue healing can take place.
Healing and the phase remedies
[BioMed, Dewit-Leunis, Piterà, Piterà2, Rozencwajg]
According to both homotoxicology and gemmotherapy, the progression of a disease can be described as a passage from left to right within the phase table (in homotoxicology we speak of progressive vicariation), while the healing necessarily corresponds to a passage in the reverse direction (regressive vicariation). It should be noted that in homotoxicology the direction of the vicariation also has a component of passage “through” the embryonic sheets.
In the initial phases (before the regulation/compensation division and therefore before the onset of chronic inflammation processes) spontaneous and complete recovery of functions and healing of tissues are possible, while in the subsequent phases there is a need for support which becomes increasingly important.
In the excretion phase, according to homotoxicology, drainage and detoxification can accelerate physiological processes and reduce the likelihood of recurrence. It is clear that, in this phase, the use of “pure” astringents can be counterproductive, at least in the first instance, as it can block the expulsion of the pathogen. Surely, if the condition tends to persist (eg., chronic diarrhea), the use of astringents may be necessary. Acute vomiting and diarrhea usually require, at best, only replenishment of fluids and electrolytes.
In the inflammation phase, according to homotoxicology, since the innate immune response is activated, immunomodulation is necessary or at least recommended. In mild and acute conditions, drainage and detoxification may be optional, but become necessary if there are relapses. Remind that suppressing fever and acute inflammation with allopathic drugs, such as anti-inflammatory, antipyretic or antitussive, can be counterproductive, because it can lead to a progressive vicarization and so to a more advanced phase of the disease.
Also for the deposition phase homotoxicology suggests the mixed approach of drainage and detoxification (which, together, constitute the first of the so-called pillars of homotoxicology) and of immunological support (second pillar), as homotoxins are located mainly in the extracellular space and the cells are not yet affected.
According to homotoxicology, resorting to the third pillar (that is, to remedies aimed at providing support to cells and organs) is envisaged for all phases to the right of the regulation/compensation division.
Gemmotherapy provides specific remedies for each of the phases.
Homeopathic miasms and tissue phases
Hahnemannian homeopathic miasms can be surely compared to tissue phases. Certainly it is not easy to establish an exact correspondence, also because homeopathic miasms are morbid tendencies (diathesis) that cannot be characterized in terms of the same parameters used to define tissue phases (at least in gemmotherapy).
Let’s start by considering that miasms, being related to chronic diseases, must necessarily be positioned to the right of the regulation/compensation division.
The psoric miasm is mostly characterized by a state of continuous struggle and hyporeaction, therefore by tiredness (the body does not have all the resources necessary for optimal functioning or for the rapid resolution of whichever problem), and by the appearance of skin rashes: there is still a detoxification reaction (through the skin), which however is not decisive because the body does not have all the resources necessary to cope with the aggression.
Some authors distinguish between a latent psora which corresponds to a chronic reactive potential without manifestations (except dysfunctional hyporeactivity) and a manifest psora which coincides with a chronic “overt” reactive pathological state (eruptions).
After the encounter with a noxa, if the inflammatory reaction is not sufficient to eliminate the pathogen[xxviii], the body ends up in a situation of disadvantage, of “weakness”, and is forced to perform a progressive vicariation that brings it into a state of persistent “fight” (indeed, even in the deposition phase there is an αβ activation) but also of hyporeaction (in fact the attack by the noxa is not resolved nor do manifest symptoms appear: it almost seems that the body has, at least temporarily, stopped reacting). This condition, which we can define, for what has been said, of “persistent hyporeaction” and which certainly is still spontaneously reversible at the beginning, has most of the typical characteristics of psora but is not yet psora. The latter, in fact, occurs only if and when the process that generated the condition continues up to the point it becomes chronic and the body activates the additional reactive (so to say, “maintenance”) mechanism that involves antibodies (γ-globulins).
So, there is a marked “similarity” between the state of “persistent hyporeaction”, reversible and characterized by hypofunction without further external manifestations, the deposition phase and the concept of latent psora. For this reason, it is natural to make these three conditions correspond.
The condition of manifest psora is established when the body begins to reactivate the inflammatory and eliminatory processes, leading to the appearance of skin rashes and of all the typical symptoms of manifest psora. It is at this moment that the regulation/compensation division is crossed, effectively entering the field of chronic diseases in the strict sense. Obviously, the manifest psora must precede, in the sense of temporal evolution, all the other Hahnemannian miasms, so it must be positioned immediately after the regulation/compensation division.
The impregnation phase is characterized by a hyperplastic tissue protein degradation (collagenosis) which is more typical of sycosis than psora. The sycotic miasma, therefore, fully corresponds to the impregnation phase[xxix], characterized by tissue protein degradation and possible hyperplasia/hyperactivity[xxx].
If it is true that the psoric miasm is not specifically characterized by collagenosis, it is also likely that this phenomenon is not completely absent in this miasm, given that, as we know from gemmotherapy and homotoxicology, protein degradation begins soon after the regulation/compensation division, as soon as the context of chronic diseases is entered (and psora is the first of the chronic conditions). Certainly this protein degradation has an evolution, in a pejorative sense, as we proceed towards the right in the table and formally along the time line.
We can, therefore, imagine that there is a certain time window[xxxi] between the onset of the chronic reaction, of a more purely psoric competence, and the moment in which the tissue protein degradation becomes so characteristic and important (from the point of view of clinical manifestations) that we can speak frankly of sycosis. For this reason, in tab. 1 psora and sycosis have been placed in sequence, but without making them exactly coincide with the phases of fibrinosis and hyalinosis. Nothing keeps us from hypothesizing that this correspondence exists and can be exact, but such a hypothesis should be verified experimentally.
The deposition phase is characterized by deposition into tissues (and therefore by hypertrophy, rather than by hyperplasia) without the “hot” phenomena due to the inflammation typical of chronic miasms (this is probably the “origin” of Grauvogl’s hydrogenoid constitution). If in this phase any possible melancholic “deposits” are exclusively produced by the “consolidation” of the accumulated phlegm, in the case of psora and sycosis the heat of chronic inflammation first produces an “adust” Phlegm and then also melancholic slags, in a sort of tissue “combustion”.
The degeneration phase is clearly of luetic type and is characterized by a degenerative hypoplasia. The dedifferentiation phase, of a completely dysplastic/dystrophic nature, can be made to correspond with the cancer miasm (we are looking for that perfection that from a tissutal point of view has been lost due to the dysplastic process).
Clearly, all the other non-Hahnemannian miasms (not mentioned here) can be seen as mixed reactive modalities, definable as intermediate between the miasms herein discussed.
Substantial identity between physical and psycho-emotional noxae
We have seen that the onset of pathologies can always be described in terms of the body’s encounter with a noxa, be it either external or internal, and of the body’s reaction to this encounter.
The word noxa is usually used to mean a “physical” agent (i.e., a microorganism, an adverse atmospheric event or a certain type of toxins that is, for example, of metabolic origin). However, psycho-emotional phenomena can also be cause of the onset of certain organic pathologies: let’s think, for example, of prolonged stress that can cause an immune deficiency, or of all those somatization phenomena that can cause both functional and (sometimes) structural problems[xxxii].
Therefore, we can affirm that there is a substantial identity between physical noxae and psycho-emotional problems with respect to the possibility of inducing body reactions. Clearly, the specific modes of reaction and the tissues/districts involved are typically different. For example, if the cold induces reactions mainly in the ENT and pulmonary system and the hepatitis virus affects the liver, a prolonged psycho-emotional distress can affect organs that are “reactively related” to the specific distress (thus causing, for example, gastroduodenitis, IBS, prostatodynia/vulvodynia, etc.).
In this document, therefore, we will speak indiscriminately of noxae, in reference both to physical etiological agents (material, such as microorganisms, or immaterial, such as the atmospheric weather) and to negative psycho-emotional situations. Obviously the psycho-emotional noxae are always considered “internal” noxae.
Psycho-emotional and physical noxae are similar also with respect to the modalities of disease causation and progression: if an external physical agent can lead to an energetic/reactive deficit (e.g., lowering of immunity) or to an acute or chronic inflammation, so too, for example, a trauma can do. For this reason, the above description of the progression of chronic diseases and the phase table are still valid for psycho-emotional problems (albeit with the due differences with respect to the modalities and affected tissues).
Even homotoxicology deals with psychic problems similarly to physical ones, so much so that they are reported in some editions of Reckeweg’s phase table.
Tab. 2 shows the stages of progression of chronic diseases in the case of psycho-emotional etiology. To simplify, we use in this text the same phase names used in homotoxicology, albeit with some difference in the “semantics” of the specific phases.
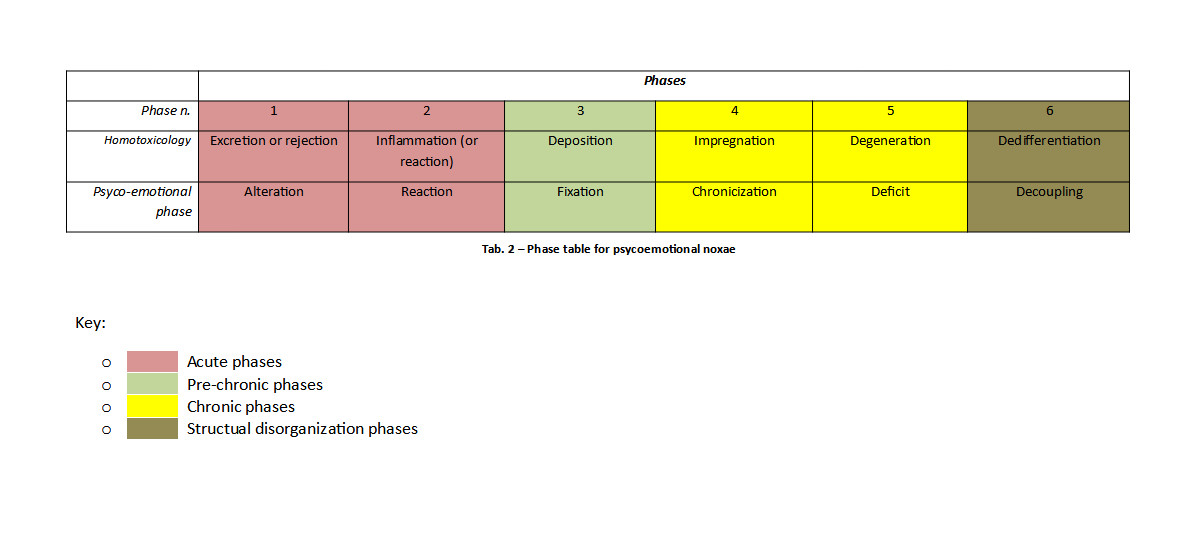
In particular:
- The alteration phase is mostly characterized by extemporaneous reactions of limited duration in time that leave no traces in the body (e.g., a fear that is overcome without leaving anything other than, at most, a non-traumatic memory). Homotoxicology classifies in this phase: functional mental disorders and “nervousness”[xxxiii].
- The reaction phase is characterized by a stronger psychosomatic reaction that lasts some time and that ceases without leaving important traces when the stimulus ceases or shortly after. For example, the fear of an examination causes some changes in the somatopsychic “tissue”, including tachycardia, intestinal troubles, decreased immunity, etc.: once the examination is over, also the reaction ceases, except, at most, for a transient period during which some “inflammatory”/excretory activity is still present, in order for the body to get rid of the reaction catabolites and any excesses of cytokines or hormones (post-examination fever or headache, “weekend syndrome”, etc.). Homotoxicology classifies in this phase: the reactive depressive syndrome and the “hyperkinetic syndrome” (roughly corresponding to ADHD according to [DSM-5], although ADHD has no limited duration in time).
- The fixation phase includes all those disturbances that produce a stable “deposition” of a content both in the individual’s memory (which we can see as a sort of mnestic “tissue”), and at the physical level (that is, a translation of the psycho-emotional content on the physical body). To this phase, therefore, belong the “removal” of trauma, the fixation of ideas and beliefs, the somatization disorders and also the phenomenon often referred to with the term “encystation” (or “crystallization”), that is the localization, within a tissue (mostly a fascial district or an organ – primary deposition process):
- of one or more “held” emotions
- of the memory of a trauma
- of chronic tension and contractures.
It is important to note that no chronic reactive (“inflammatory”) phenomenon, either somatic or psycho-emotional, is associated with this incystation, except, at most, in the event that the affected tissue is stimulated. We can imagine, for example, a distortion of the fascial tissue or a chronic contracture that are not painful (sensations below the threshold of consciousness). Homotoxicology puts in this phase: psychosomatosis (now classified as somatic symptom disorders and related disorders, according to [DSM-5]), neuroses (differently reclassified on the basis of clinical symptoms), phobias (anxiety disorders according to [DSM-5]), neurotic depression (dysthymia according to [DSM-5]).
- During the chronic phase, the first morpho-functional and secretory changes begin to appear: changes in the concentrations and management of neurotransmitters, increase in inflammatory cytokines, changes in blood flow in specific regions of the nervous system, meiopragias[xxxiv], structural alterations of specific loci (e.g., enlargement of the lateral ventricles in major depression accompanied by psychosis). This phase includes all those disorders that could be thought of as secondary inflammation responses consequent to the fixation phase.
- The deficit phase includes all those disorders that are characterized by a functional deficit, possibly accompanied by tissue degeneration that is secondary to or concomitant with the prolonged morpho-functional and secretory alteration of the chronicization phase. Homotoxicology here includes: schizophrenia and mental deficits.
- The decoupling phase includes, in homotoxicology: mania and catatonia.
References
|
[Andrianne] |
Philippe Andrianne, “Les bases de la prescription en gemmothérapie: paramètres biologiques sériques et phytosociologie”, Phytothérapie 6, 301–305 (2008) (DOI: 10.1007/s10298-008-0344-9) |
|
[BioMed] |
http://www.biologicalmedicine.info/homo.htm (Retrieved: 2017-11-13) |
|
[Cheng] |
Hui Cheng et al., “New paradigms on hematopoietic stem cell differentiation”, Protein Cell 2020, 11(1):34–44 |
|
[Crame] |
Thorsten Crame et al., “HIF-1α Is Essential for Myeloid Cell-Mediated Inflammation”, Cell, (112), 645–657, 2003 |
|
[Dewit-Leunis] |
Serge Dewit, Jean-Claude Leunis, “Trattato Teorico e Pratico di Fitoterapia Ciclica”, Nova Scripta, Genova (2018) |
|
[Dixon] |
Dixon et al., “Kupffer Cells in the Liver”, Compr Physiol. 2013 April; 3(2): 785–797. doi:10.1002/cphy.c120026. |
|
[DSM-5] |
American Psychiatric Association, “Diagnostic and Statistical Manual of Mental Disorders”, Fifth Edition (DSM-5) |
|
[Häggström] |
Immage by A. Rad and Mikael Häggström, M.D.- Author info – Reusing images – Image:Hematopoiesis (human) diagram.png by A. Rad, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=7351905 |
|
[Heel] |
“Routine Therapy – The Practitioner’s Handbook of Homotoxicology”, Heel USA, 3.rd US edition (2010) |
|
[Henry] |
Pol Henry, “Gemmoterapia”, Giuseppe Maria Ricchiuto Editore (1989) |
|
[Matsuzaki] |
Shinichi Matsuzaki et al., “Extracellular acidification induces connective tissue growth factor production through proton-sensing receptor OGR1 in human airway smooth muscle cells”, Biochemical and Biophysical Research Communications, 413,499–503 (2011) |
|
[Öörni] |
Katariina Öörni et al., “Acidification of the intimal fluid: the perfect storm for atherogenesis”, J. Lipid Res. 56: 203–214 (2015) |
|
[Piterà] |
Fernando Piterà, “Compedio di Gemmoterapia Clinica”, 6a edizione, Ed. De Ferrari (2007) |
|
[Piterà2] |
Fernando Piterà, Marcello Nicoletti, “Gemmoterapia – Fondamenti Scientifici della moderna Meristemoterapia”, Nuova Ipsa Editore (2016) |
|
[Reckeweg] |
Hans-Heinrich Reckeweg, “Materia Medica”, 4th edition, Aurelia Press |
|
[Roggel] |
Roggel et al., “Role of Kupffer cells in host defense and liver disease”, Liver International 2006; 26: 1175–1186 |
|
[Rozencwajg] |
Joe Rozencwajg, “Dynamic Gemmotherapy”, Emryss Publishers (2013) |
|
[Sluimer] |
Judith C. Sluimer et al., “Hypoxia, Hypoxia-Inducible Transcription Factor, and Macrophages in Human Atherosclerotic Plaques Are Correlated With Intraplaque Angiogenesis”, JACC 51(13), 2008, 1258-1265, doi:10.1016/j.jacc.2007.12.025 |
|
[Tetau] |
Max Tétau, “Gemmoterapia – Nuovi studi clinici”, Nuova Ipsa (2001) |
|
[Walmsley] |
Sarah R. Walmsley et al., “Hypoxia-induced neutrophil survival is mediated by HIF-1α-dependent NF-κB activity”, JEM, 201(1), 2005, 105–115; doi: 10.1084/jem.20040624 |
|
[Wikipedia] |
http://*.wikipedia.org |
|
[Winer] |
Winer et al., “B Lymphocytes Promote Insulin Resistance through Modulation of T Lymphocytes and Production of Pathogenic IgG Antibody”, Nat Med. 2011 May; 17(5): 610–617 |
Notes
[i] Also called haemocytoblasts: this term actually refers to a now (at least partially) outdated model, according to which haemocytoblasts derive from undifferentiated mesenchymal elements called haemoistioblasts. However, the nomenclature is maintained in several texts.
[ii] They are called granulocytes because they are characterized by the presence of granules in the cytoplasm, and polymorphonuclear because their nucleus has a variable shape and is usually divided into three lobes.
[iii] Both granulocytes and cells of the histio-monocyte lineage (monocytes and derivatives, macrophages and dendritic cells) are capable of phagocytosis, therefore the term phagocytes includes both cell lines. Here with microcytic phagocytosis, the original author of the expression [Piterà] refers to the phagocytosis exerted by granulocytes, that are smaller than macrophages and monocytes.
[iv] α-globulins are synthesized by hepatocytes, responsible for the production of proteins of the inflammatory phase (including PCR and, indeed, the α-globulins). Note that, according to the Hippocratic-Galenic medicine, the liver manages Bile, the humor responsible of inflammation processes.
[v] Liquid phase immunoprecipitation.
[vi] See [Henry] p. 26. Fibrinous exudation is not to be confused with the fibrinous phase (see below): the phenomenon of fibrin deposition is due to the “spontaneous” degeneration of the exudate rather than to a deposition due to a chronic hyper-αβ or even hyper-αγ state.
[vii] Although the name may suggest the opposite, no organ steatosis occurs during the steatosis phase.
[viii] He only mentions the hyper-β fraction, linked above all to connective tissue, and a “lesion” of such tissue, which marks the onset of chronic inflammation (he probably refers, here, to the beginning of the “competence” of γ proteins).
[ix] Both the activation phase and the exudative inflammation phase involve hypersecretion, but in the first case this is not produced as a result of inflammation, while in the second it is, so much so that Pol Henry himself tells that the hyper-α fraction is specifically linked to acute inflammation and leukocytes. Clearly, here we are trying to formally distinguish phases that in real cases tend to blur without sharply distinguishing from one another.
[x] In Dewit’s and Leunis’ model, the concentration of lipidic and proteic macromolecules in the serum begins to be too high for these molecules to remain in solution; therefore they precipitate and deposit in the tissues and, so, in the organs. In this model, the deposition of noxae into the tissues is not contemplated, at least explicitly, as is the case in homotoxicology.
[xi] A point or place characterized by a lesser resistance.
[xii] Unlike gemmotherapy, homotoxicology does not refer to measurable biological parameters.
[xiii] Lymphoplasmacytes are typical of chronic inflammation and the gamma fraction. (see [Henry], page 26).
[xiv] Note the correspondence with the regulation/compensation division line of homotoxicology.
[xv] In this box, the word fibrosis specifically refers to the phenomenon of tissue fibrosis, that is, the thickening of connective tissue, not to Dewit’s and Leunis’ fibrosis phase.
[xvi] Let’s think, for example, of what happens in the onset of type 2 diabetes: the adipose cells increasingly “full” of fat, begin to react to this saturation by producing inflammatory cytokines which, in turn, trigger the process that eventually leads to insulin resistance and therefore to diabetes. In this process, (at least in some cases) γ-globulins are produced by the body in response to the accumulation of adipose deposits [Winer].
[xvii] Which is in fact a local accumulation of blood, or if we prefer a “stagnation” of blood, not to be confused with the condition of the Blood Stagnation of Chinese medicine.
[xviii] Archaic word that means cooking.
[xix] Think of fire that burns wood and dries up all its liquids, producing coal, that is dry, hard and black.
[xx] The thickened Phlegm typical of the deposition phase is sometimes found in Traditional Chinese Medicine described as “Phlegm invading the collateral vessels”.
[xxi] But also to the Traditional Chinese Medicine.
[xxii] Or rather on its power relatively to the body’s defense and reaction capabilities.
[xxiii] Liver cirrhosis, for example, is a chronic liver disease characterized by the formation of fibrous tissue and subsequent necrosis of the parenchyma, infiltration of inflammatory and connective cells that form phlogistic scar structures, and subsequent nodular regeneration of the parenchyma. The initial (asymptomatic) stage of the disease is called compensated cirrhosis; the stage with a manifest clinical picture is called decompensated cirrhosis. On electrophoresis, typical signs are the decrease in α1-antitrypsin, the decrease in albumin and the increase in γ-globulins.
[xxiv] Cirrhosis is already to be considered in phase V (necrotic) according to Table 3 of [Dewit-Leunis], in partial disagreement with the algorithm on page 24 of the same text.
[xxv] Melancholia deficiency (hypostructuring) and Melancholia excess (hyperstructuring) are both “perverted” conditions. But Melancholia, in addition to being perverse in quantity, can also be perverse in quality: let’s think, for example, of Melancholia which is generated by the “cooking” of correct humors (see, for example, the Unani-Tibb concepts of malankholia damvi produced from the combustion of the Blood, malankholia safravi produced by the combustion of the Yellow Bile, malankholia balghami produced by the combustion of Phlegm and malankholia saudawi produced by the combustion of the corrected Melancholia).
[xxvi] For example, this implies that the remedies provided by both models can be used for each phase.
[xxvii] See, for example, the slightly different views regarding the placement of the hyper-α and hyper-β phases in the paragraph “Inflammation phase”.
[xxviii] Or if the symptoms are suppressed with drugs.
[xxix] Reckeweg himself defines Thuja, the main remedy of sycosis, a remedy for the retoxic impregnation phases [Reckeweg].
[xxx] The heat of the renewed immune reactivity can be thought of as somewhat related to the psycho-physical hyperactivity typical of this phase.
[xxxi] Here we consider sycosis chronologically subsequent to psora, but clearly this only holds formally, since the former is certainly a more “advanced” condition, from the point of view of tissue damage, than the latter.
[xxxii] Chronic contraction of the pelvic floor muscles, for example, can cause disorders such as prostatodynia and vulvodynia, which can be characterized not only by pain, but also by tissue inflammation with alterations in blood parameters (such as PSA). This tissue inflammation, in turn, can lead to fibrotic phenomena (deposition) and to structural and – therefore – functional alteration of the affected organ.
[xxxiii] The terms used in homotoxicology in relation to mental disorders are rather old and do not correspond to the current ones (as defined in DSM-V [DSM-5], at the time of writing of this text).
[xxxiv] Decrease in the functional activity and reactive capabilities of an organ.



